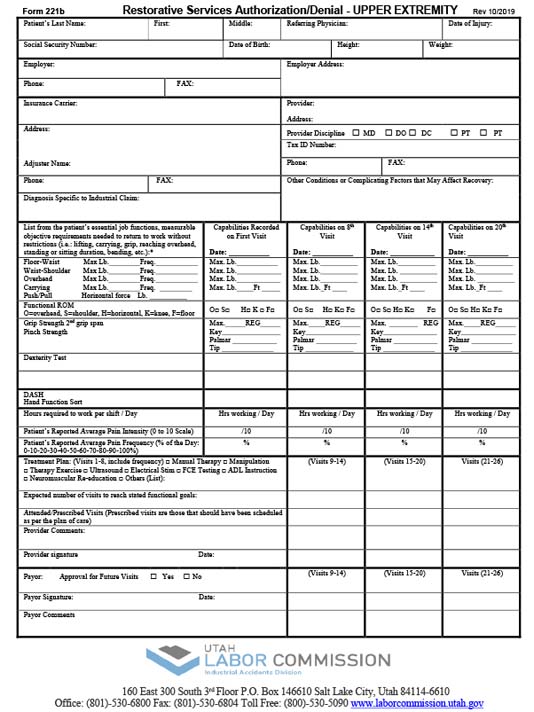
Form 221b – Upper Extremity Restorative Services Authorization/Denial
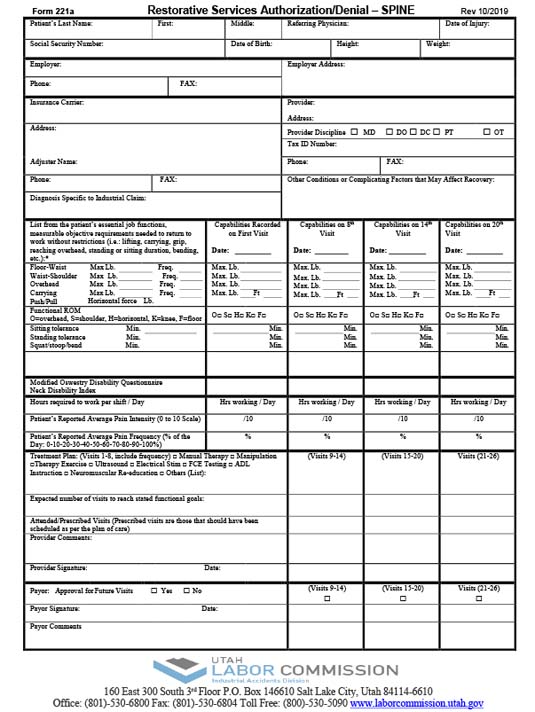
Form 221a – Spine Injury Restorative Services Authorization/Denial
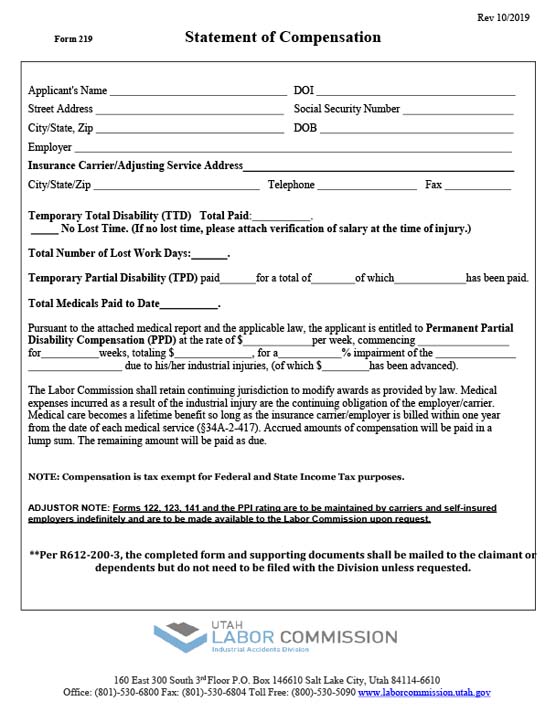
Form 219 – Permanent Partial Disability Statement of Compensation
Form 123 – Physician’s Initial Report of Work Injury or Occupational Disease
Form 102 – Application to Change Doctors
Form 044 – Employee’s Notification of Intent to Leave Locality or State, and to Change Doctor or Hospital
Form 043 – Attending Physician’s Statement
Form 441 – Insurance Carriers/Self Insurer’s Notice of Further Investigation of a Workers’ Compensation Claim
Form 142 – Statement of Insurance Carrier or Self Insurer With Respect to Discontinuance of Benefits
Form 142 – Statement of Insurance Carrier or Self Insurer With Respect to Discontinuance of Benefits
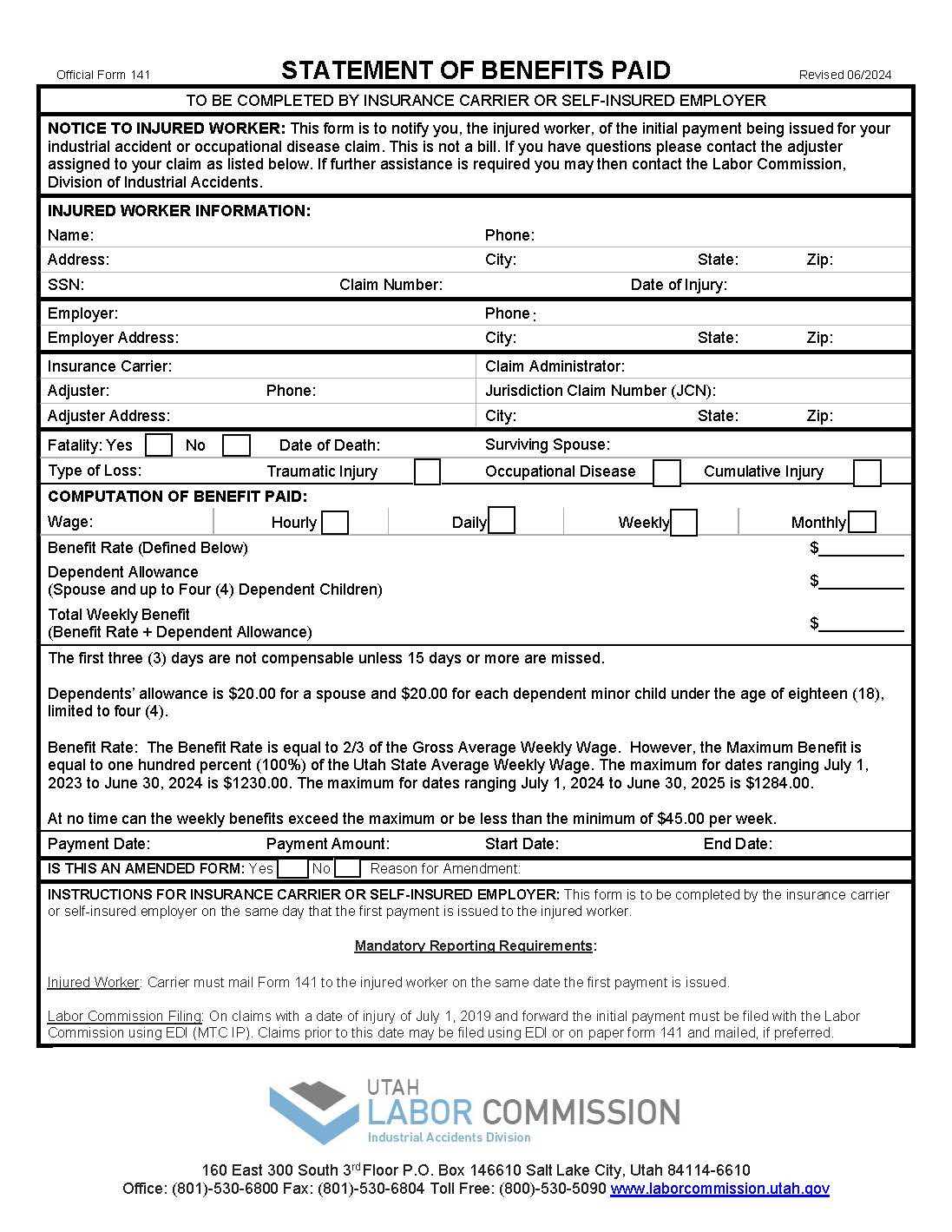
Form 141 – Initial Statement of Insurance Carrier or Self Insurer With Respect to Payment of Benefits