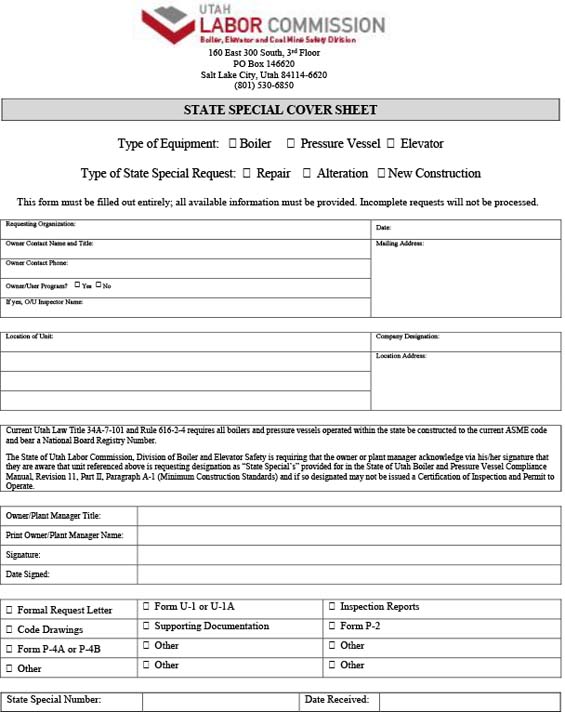
Special Design Plan Cover Sheet
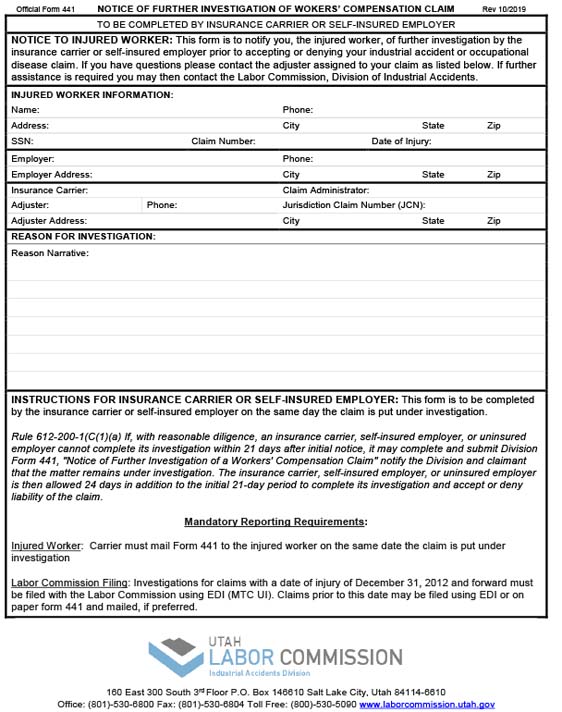
Form 441 – Insurance Carriers/Self Insurer’s Notice of Further Investigation of a Workers’ Compensation Claim
Form 142 – Statement of Insurance Carrier or Self Insurer With Respect to Discontinuance of Benefits
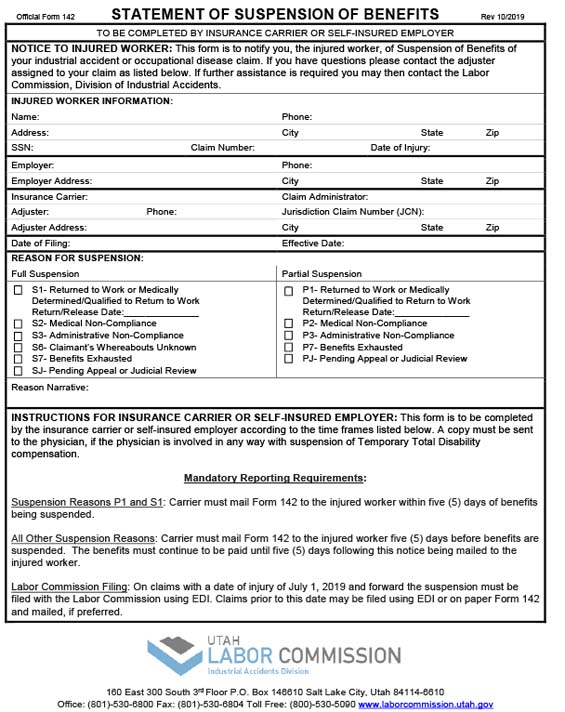
Form 142 – Statement of Insurance Carrier or Self Insurer With Respect to Discontinuance of Benefits
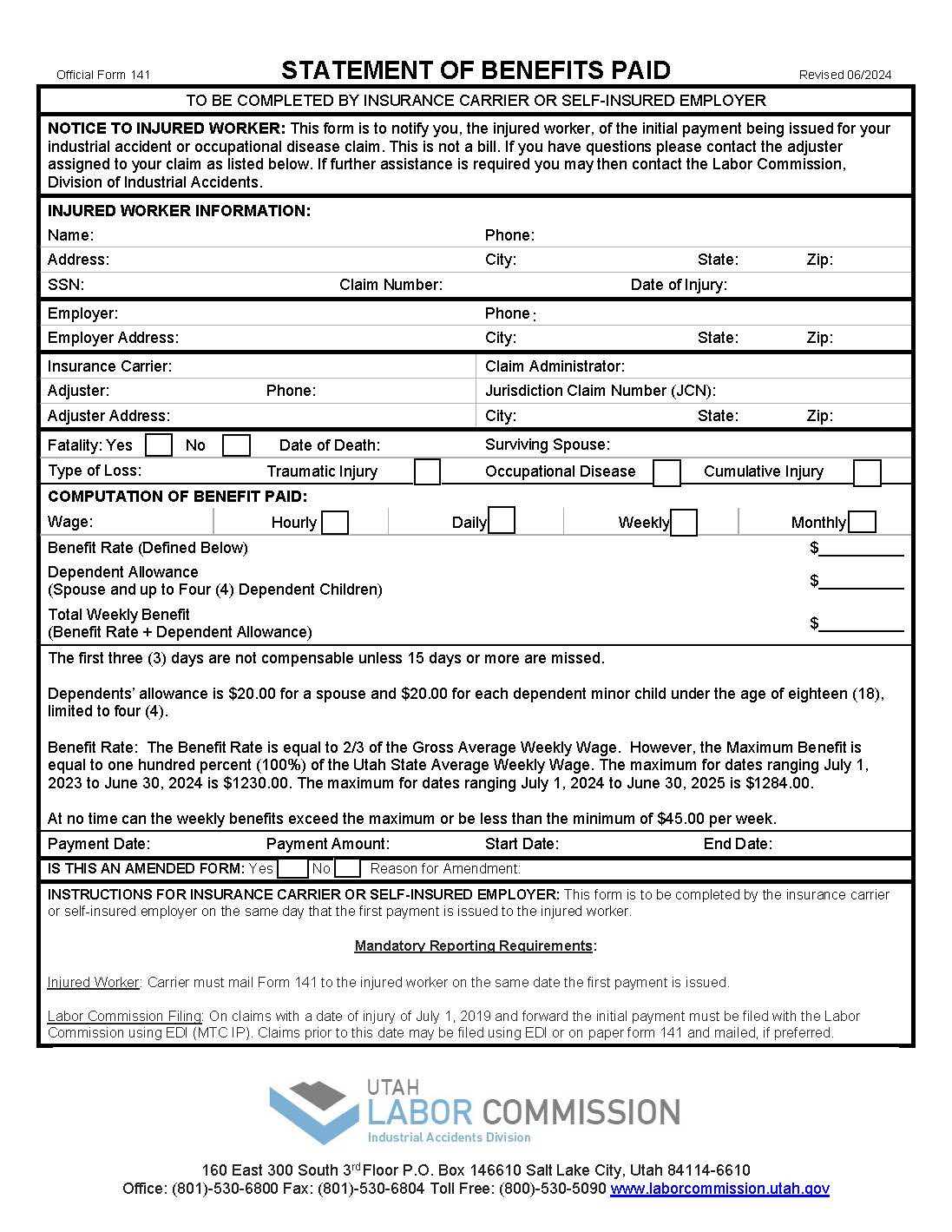
Form 141 – Initial Statement of Insurance Carrier or Self Insurer With Respect to Payment of Benefits
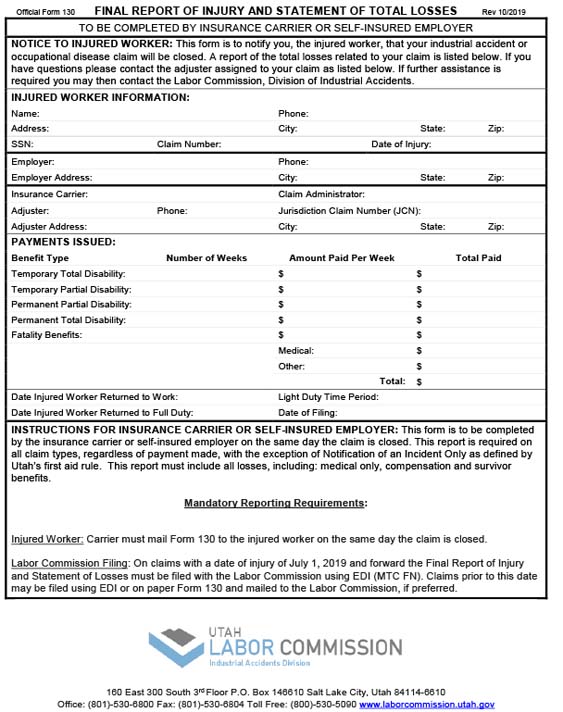
Form 130 – Insurance Company’s and Self Insurer’s Final Report of Injury and Statement of Total Losses
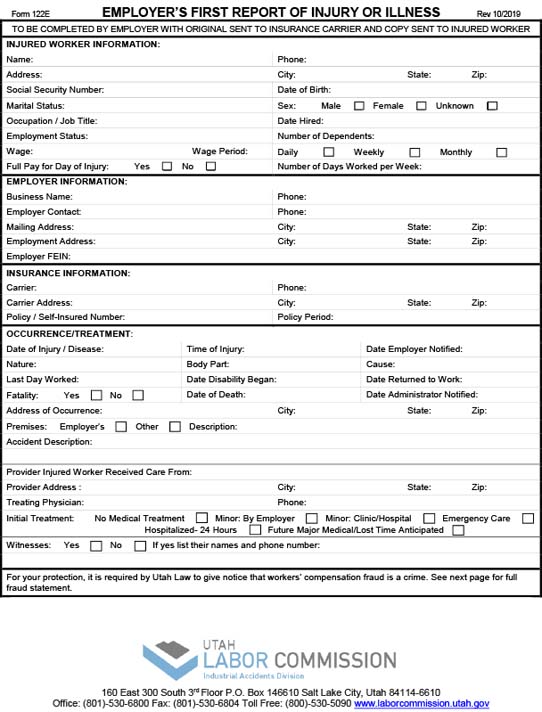
Form 122 E – Employers First Report Of Injury or Illness
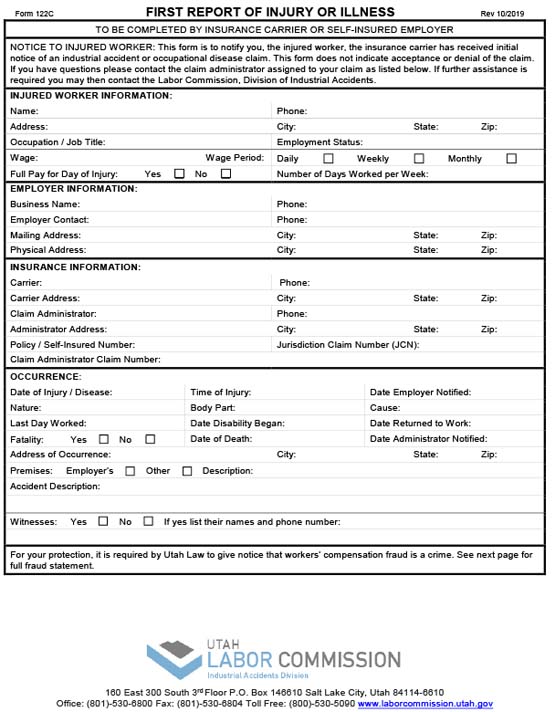
Form 122 C – Insurance Carrier/Self Insured Employer First Report of Injury or Illness
Form 100 – Injured Workers’ Rights and Responsibilities (Spanish)
Form 100 – Injured Workers’ Rights and Responsibilities
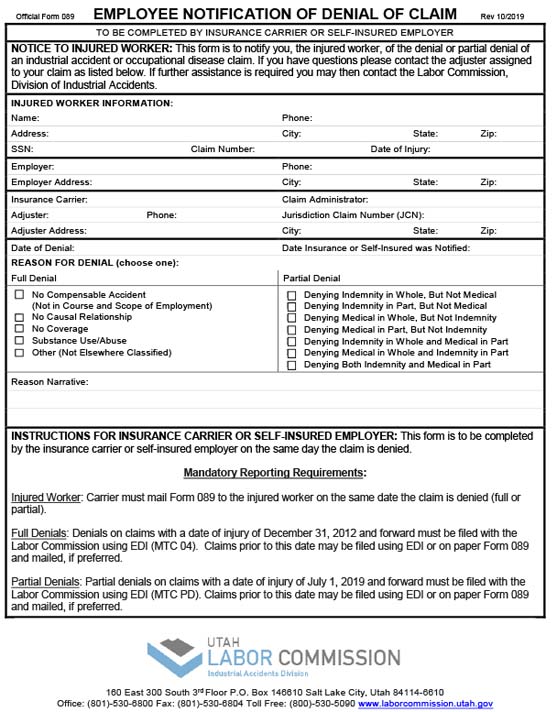
Form 089 – Employee Notification of Denial or Partial Denial of Claim